
SDOH Clinical Care
0.0.4C1 - CI Build
SDOH Clinical Care
0.0.4C1 - CI Build
SDOH Clinical Care - Local Development build (v0.0.4C1). See the Directory of published versions
Previous Page - Gravity Project Background
The Gravity Project focus on defining coded content to support three priority social domains, food insecurity, housing instability and homelessness, and transportation access.
 |
The Gravity Project will not focus on evaluating, testing, or harmonizing existing social risk screening tools and instruments, nor will it identify social risk data elements that do not directly support one of the three priority social domains previously listed in the Scope Statement. This project also will not validate or provide incentives for implementation of the identified SDOH data elements.
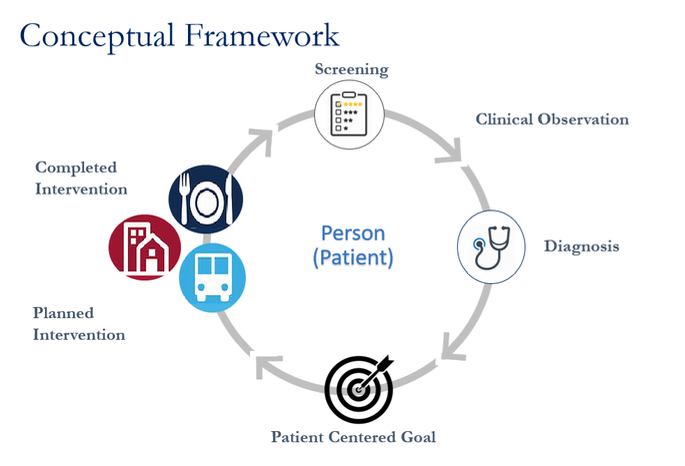
Coded SDOH content is captured across four core health care activities: screening, assessment/diagnosis, goal setting, and interventions. The conceptual framework illustrated below shows how these activities form a cycle of care. Over time, as additional screening and assessment is performed, a patients progress toward care goals can be tracked and measured.
 |
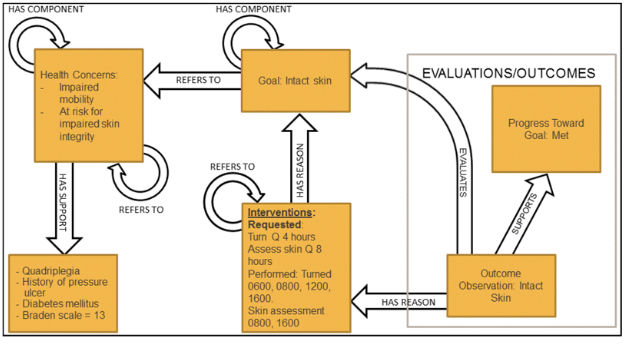
The figure below was derived from the HL7 Patient Care WG Domain Analysis model for Care Plan information. It informs the design of the FHIR Resources used in this IG.
 |
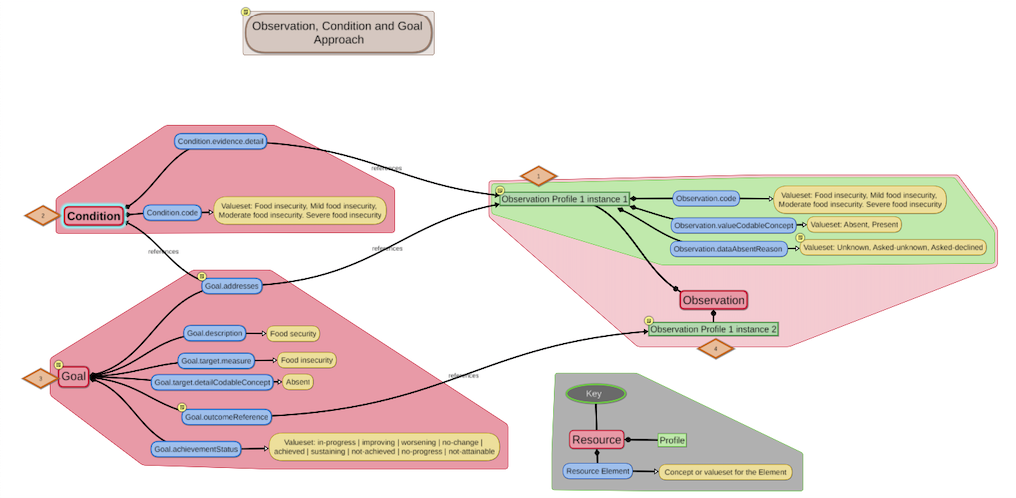
The relationships between the various types of information are supported by the designs developed for the resources. The diagram below shows the data model for the assessment observation, condition (diagnosis), and goal (patient centered goal). The semantics designed for the profiled resources support the envisioned cycles of assessment, diagnosis, and goal setting. The mind map illustration represents profiles developed in this IG for the FHIR Observation, Condition, and Goal Resources. It shows instances of profiled Resources that would be used over time as part of an iterative care process.
 |
The data modeling includes additional considerations specified using FHIR Path expressions.
| Profile | Additional Constraints |
|---|---|
| Observation Profile 1 Example 1 | Food insecurity observation that is the result of clinical assessment based on information collected in the screening questionnaire and other information gathered during the encounter. 1) Allows an Observation that specifies Food insecurity absent (aka Food Security), Mild food insecurity, Moderate food insecurity, Severe Food insecurity, or Food insecurity, unknown. 2) xpath rules could specify xpath that must either Observation.valueCodableConcept or Observation.dataAbsentReason, but not both, must be provided. |
| Condition | Allows a Condition that specifies Mild food insecurity, Moderate food insecurity, Severe Food insecurity. |
| Goal | Patient-centered goal documenting the desired outcome of planned interventions. |
| Observation Profile 1 Example 2 | Food insecurity observation that is the result of a post-goal, post-intervention evaluation/assessment. |
The FHIR CarePlan Resource is at a Maturity Level 2 and a number of issues remain to be resolved before the SDOHCC_CarePlan_FoodInsecurity profile(s) can be considered. This includes comparing SDOHCC requirements to the profiling of the CarePlan Resource done in the US Core IG.
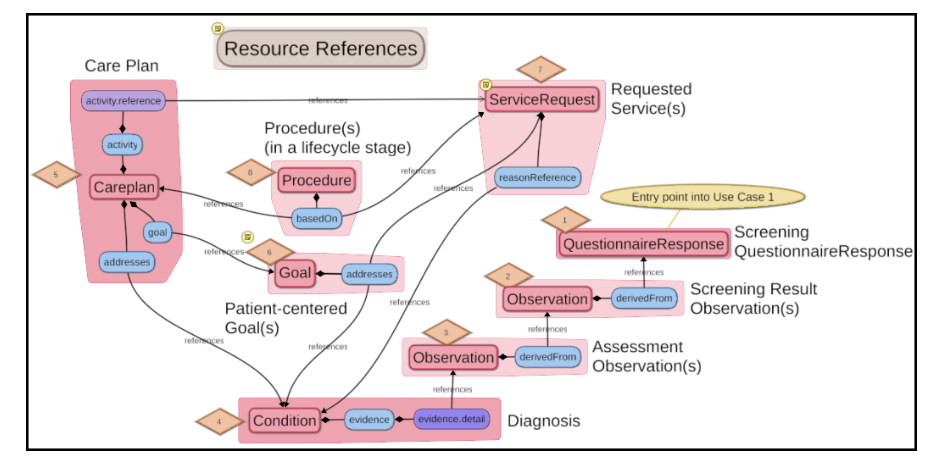
The diagram below is intended to show Resources that reference or are referenced by CarePlan as the patient progresses from:
Each time the resources referenced by the CarePlan are updated/versioned, the information that would be retrieved if the CarePlan resource was retrieved will be updated. A CarePlan resource functions as a “dynamic resource” countinuously pointing to the “current” view of the patient’s plan. Snapshots of the CarePlan resource may need to be instantiated as a document to be preserved at a specific point in time to facilitate signature and sharing of the information with other parties as points in time.
 |
Once this profile is created, additional guidance will be provided on
IG © 2020+ HL7 International - Patient Care WG. Package hl7.fhir.us.sdohcc#0.0.4C1 based on FHIR 4.0.1. Generated 2020-05-14
Links: Table of Contents |
QA Report
| Version History  |
|
 |
Propose a change
|
Propose a change